Global Journal of Medical & Clinical Case Reports & Studies
Volume 1, Issue 1, April 2023, Pages: 01-20
Received: October 13th, 2022, Reviewed: November 3rd, 2022, Accepted: November 13th, 2022, Published: April 03, 2023
Global Journal of Medical & Clinical Case Reports & Studies 1(1) 1-20
Authors: Suha Matar, PGD,CPHRM,RN¹*, Mohammad T. Abuawwad², Mohammad J. J. Taha², Ayham R. K. Sara², 4 Rakan Munif Nassralla²
¹Faculty of Medicine, Health Management (leadership)PGD, CAPE Town university, Cape Town, South Africa
²Faculty of Medicine, Cairo University, Cairo, Egypt
*Corresponding Author:
Name: Suha Matar
Keywords: Home Health-Care, Palliative Care, Telehealth, COVID-19, Saudi Arabia, SARS-CoV-2
ABSTRACT:
Home Healthcare (HHC) is defined as in-home delivery of care by a licensed worker in a patient’s home. This includes many services such as skilled nursing, physical and occupational therapy, nutritional, medico-social and laboratory pharmaceutical services, etc. It is considered an important component of the healthcare sector and one that presents a distinct set of decision problems for healthcare providers. The importance of HHC is increasing due to social and economic factors that have helped its expansion.
The recent increase in life expectancy of the general population influenced the demand for HHC. HHC allows for improvements in the quality of life for patients and reduction of recovery periods of illness.
According to the World Health Organization (WHO), COVID-19 disease is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and declared its outbreak a Public Health Emergency of International Concern (PHEIC) on January 30, 2020. It was declared a pandemic on March 11, 2020. The pandemic increase demand for HHC both quantitatively and qualitatively, the Kingdom of Saudi Arabia (KSA) was not an exception, for workforce and development in HHC became of critical importance. In an effort to control the spread of COVID-19 infection, KSA enforced a very restricted curfew, during which; a patient was unable to attend to a hospital, further increasing demand on HHC services. In KSA, although many efforts to improve the health sector are in progress as a part of the 2030 Vision program, it still requires further development and expansion, especially when it comes to HHC. Starting in 1991 with the first HHC program, KSA has only 2262 HHC nurses and 2 HHC programs among its ministry of health today.
1. Introduction
Home health-care (HHC) is clinical medical care services provided by nurses, occupational therapists, physical therapists, or other skilled medical professionals at the home of the patient which is linked to the care plan following the patient’s discharge after hospitalization [1]. Under the HHC category falls many subservices such as palliative care (PC), tele-health, online health services and many others [2].
Globally, the need for Home Health-care (HHC) programs has increased due to an increase in chronic and acute diseases which need continuous monitoring. This need becomes more evident in the elderly
population, as 70.5% of HHC patients are 65 years old or older [3]. In 2020, over 5 million cases of chronic
disease were recorded in KSA, and the number is predicted to reach 10 million by the end of 2030 [4].
In March 2020, the World Health Organization (WHO) announced the novel Corona Virus Disease79 2019 (COVID-19) as a global pandemic [5]. The first confirmed COVID-19 case in Saudi Arabia was announced on 02 March 2020 [6]. Until 31 May 2020, there have been 85,261 confirmed cases, with 62,442 total recoveries and 503 deaths. The death rate per million of the population is very low in Saudi Arabia, this could be the result of the Ministry of Health (MOH) preparedness and efforts, as it increased hospital’s capacities and provided treatment protocols [7].
In order to control the spread of the COVID-19 virus, the Saudi government took strict measures to control public interaction. The strict curfew was successful in limiting viral spread, but paused challenges to access to health-care. Therefore, an increasing demand on HHC services was established, driving the authorities as well as the private sector to embrace the availability and accessibility of HHC services [7].
In an effort to understand the impact of COVID-19 pandemic on the HHC sector, this review aims to explore the changes and challenges that occurred in the field as a result of the COVID-19 pandemic, and to assess the growth and spread of HHC in both the public and private sectors. This work also attempts at mapping the future of HHC in Saudi Arabia in the scope of 2030 vision of the Saudi government.
2. Methodology
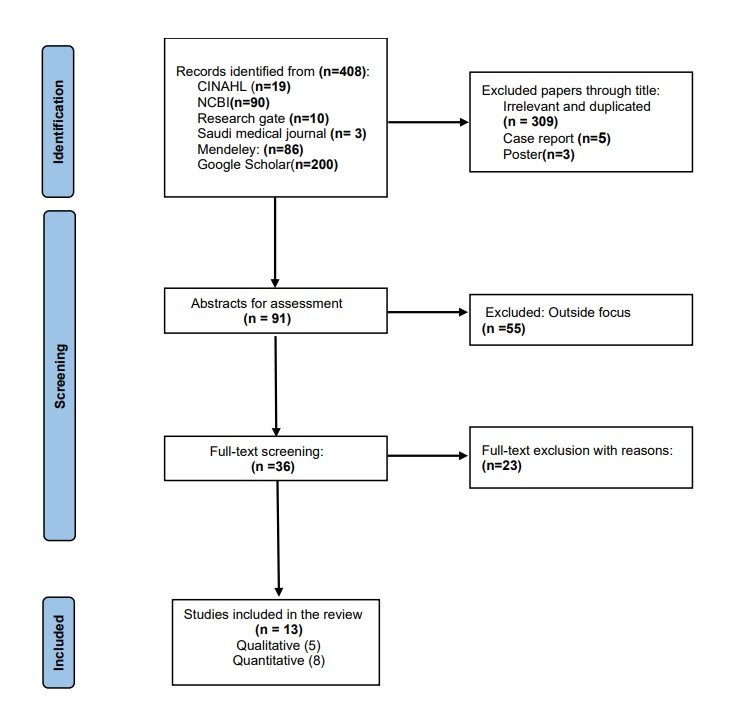
Since this is the systematic review there for an institutional board or an ethical committee approval was not required. In this systematic review, our methodology followed the Preferred Reporting Items for systematic Reviews and Meta-Analyses (PRISMA) [8]. Figure (1) summarizes these steps. Search was conducted on literature platforms (CINAHL, Research Gate, Saudi medical journal, Mendeley and Google Scholar) using “covid19”, “home health-care” and “Saudi Arabia” as main keywords, and terms like “palliative care”, “pandemic”, “SARS-CoV-2”, “KSA”, “HHC”, and “PC” as secondary terms that were toggled with main terms to ensure maximum coverage of all available research. Only papers in English were included, and they must be published after October-2019 in order to be in sync with the beginning of COVID-19 pandemic. After the initial gathering of papers, they were subjected to three stages of filtration. First, filtration by title. Second, filtration based on abstract, and finally, a full text assessment. Each stage was performed by two reviewers at least, to ensure accuracy and avoid bias or mistake. Finally, 13 articles were identified as relevant and suitable for review, 8 quantitative and 5 qualitative. And so; they were distributed among reviewers. Each article was randomly assigned to two reviewers, each of whom extracted data through a specially designed data abstraction form. Each paper was thoroughly reviewed to extract all relevant data.


Figure 1: The Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA)
3. Review of Literature:
3.1 Overview
Our search yielded 13 studies, 8 were quantitative retrospective cross-sectional studies and 5 were qualitative (2 Literature Reviews and 3 were recommendation articles). The ratio between descriptive and analytical studies reflects the trends in research and HHC development in Saudi Arabia. Studies were distributed across major cities in Saudi Arabia, with most of them located in the capital Riyadh.
As for descriptive studies, sample sizes ranged between (101-1961) according to data availability, and populations were chosen according to each study’s aim. Samples and settings for each study are summarized in table (1). Each study used a different reliable and valid scale, and all included descriptive statistics and suitable statistical analysis. Qualitative articles were specified for respective fields. One literature review introduced the novel Remotely Accessible Health-care at Home (RAHAH) connected health intervention.
Another literature review handled the knowledge and attitude towards HHC and PC in nurses of Saudi Arabia. Three articles concerned recommending guidelines and solutions for HHC and PC issues. One article provided an expert’s opinion and advice to solve the respiratory syncytial virus (RSV) vaccination reduction that was a consequence of COVID-19 restrictions. Another article discussed the training programs of HHC professionals and providers, while the last article provided a complete guideline and standardization protocol for telerehabilitation practice in Saudi Arabia.
3.2 Nursing in HHC and PC
In HHC, nursing care is the cornerstone upon which the rest of the service relies. Nurses in HHC are responsible for wound dressing, ostomy care, intravenous therapy, administering medication, monitoring the general health of patients, pain control, and other health support [19]
In Saudi Arabia, nurses face serious challenges in terms of cultural and linguistic integration [20]. Being mostly of foreign nationalities, most nurses come from different religious and cultural backgrounds, which subjects them to several barriers before they could communicate with their patients. In the HHC setting, this problem is further complicated by the technical and religious considerations regarding providing care at patient’s homes [1].
In an effort to assess nurses’ knowledge and attitude towards HHC and PC in Saudi Arabia, several studies were performed. The overall most important finding was that nurses in KSA lack the appropriate knowledge and training to provide suitable HHC and PC [1]. This was attributed to different causes which indicates the importance of the HHC and PC in Saudi Arabia.
COVID-19 adds another challenge to the situation, since the demand on HHC and PC services increased drastically in a very short period [11]. In addition, more responsibilities on HHC staff were imposed by the pandemic, this urged Saudi health professionals to start addressing the problem and try to solve it by different methods. During the pandemic, most patients preferred to avoid hospital visits out of fear of getting infected by COVID-19 which increased the burden on HHC and PC. [17, 18] Concerned themselves with standardizing HHC, PC and telehealth practices, by providing professionally designed guidelines and protocols. Also, training programs and professional guidance was provided in these articles, contributing to the formation of a new nurse culture that includes HHC, PC and telehealth proficiency.
In [1], authors noted that nurses who engaged their patients and their families were especially important in HHC. They found that nurses are more likely to report falls and their risk factors, and to assess in treatment as well. This review also found that family presence is an important need in end-life situations, thus explaining the need for further employment of HHC and PC. The Saudi population was found to be quite passive towards HHC and PC services. PC services were not fully utilized, and HHC services were even utilized to a lesser extent, this explains why PC is mainly used as an inpatient service in contrast to home-based PC which is only rarely used. It is important to note that is not due to lack of available HHC services, but because most patients prefer a hospital-based PC service.
Table 1: Summery of articles reviewed in this work
| AUTHOR | PURPOSE | SAMPLE/SETTING | DESIGN | DATA COLLECTION/MEASURES | KEY FINDINGS |
| AL AWAJI ET AL.[3] | Use of telehealth to provide SLS services after COVID-19 and the attitude towards it. | 385 Caregivers of children aged 0-14 | Quantitative retrospective Cross- sectional Online Survey | Statistical analysis of caregiver’s answers to online self-answered survey to determine tendencies | The study revealed that SLS services in Saudi Arabia are limited and that accessing these services is challenging. |
| 34% respondents agreed that video call therapy can be effective and 49% were affirmative that therapy can be provided through video. | |||||
| Respondents showed a willingness to use telehealth in therapy sessions, expressing a preference for video calls over other options. | |||||
| AL SHEHERY ET AL.[9] | Comparison between inpatient, outpatient and consultation services before and after COVID-19 | Medical records of 319 palliative care patients at KFMC | Quantitative Retrospective Cross- sectional Online Survey | Comparison of medical records for same patients at KFMC between March-June/2019 and March-June/2020 | Total admission to PC units did not decrease due to COVID-19. |
| Support was provided through a virtual clinic and telehealth. | |||||
| Around 87% of patients were fully satisfied (5/5) with the services provided by the virtual clinic. | |||||
| There were no positive COVID19 cases in our healthcare workers in the palliative care department due to the high standard precautions applied at KFMC. | |||||
| BAGHDADI ET AL.[10] | Assessment of fear levels among caregivers of children and its effect on their vaccination during COVID-19 pandemic. | 577 caregivers of children ≤ 2 years old | Quantitative Retrospective Cross- sectional | Regression analysis of answers to a self- administered online survey measuring “fear-level classifiers” | 90.8% of caregivers were mothers. |
| The prevalence of intentional vaccination delay was 37%. | |||||
| Odds of delaying scheduled childhood vaccination because of COVID-19 pandemic fears were greater among caregivers with higher levels of fear (OR 1.10, 95% CI 1.02–1.11). | |||||
| Common reasons for delaying vaccinations were COVID-19 infection and prevention of exposure to COVID-19 cases. | |||||
| ALABBASI ET AL. [11] | Investigation of the impact of HHC on mortality rates in elderly with functional difficulty. | All patients (593) who were enrolled in the HHC program in a referred medical complex, Jeddah, Saudi Arabia between the years 2017 and 2020. | Quantitative Retrospective Cross- sectional | Analysis of data obtained directly from the hospital system, which contained home care visits information. | During the 2020 pandemic, there was a sharp increase in HHC compared to previous years. |
| The most successful HHC visits were provided in 2020 compared with the year 2017, but no association between success and death rates was found. | |||||
| The study model has indicated that those who cancelled their visits more frequently had a higher risk of mortality. | |||||
| ALSHAHRANI ET AL. [12] | Assessment of fatality trends among HHC patients with chronic disease due to infection by COVID-19. | 101 patients with chronic illness at the Homecare Department in the (AFHSR), who were infected with COVID- 19 | Quantitative Retrospective Cross- sectional | Designed data collection sheet obtaining data through the hospital information healthcare system. | A high case fatality rate among homecare patients infected with COVID-19 (26.7%). Increasing with age. |
| Almost half of patients were admitted to the hospital for management of COVID-19, and hospitalized patients had significantly higher case fatality. | |||||
| A significantly high case fatality rate among homecare patients with diabetes, cerebrovascular accidents and epilepsy was found. | |||||
| AL-RAYES ET AL. [13] | Comparison of public attitude towards 937- Telephone Health Services in KSA before and during the COVID-19 pandemic. | 1961 citizens and residents of KSA | Quantitative Retrospective Cross-sectional Online Questionnaire | Web-based questionnaire distributed online through digital communication means. | An increase in awareness and utilization of 937-telephone health services across all population groups in KSA during COVID-19 Pandemic. |
| An increase in public acceptance of a telephoneaccessed health service for the population. | |||||
| Utilization of 937-telephone health services increased significantly during the COVID-19 pandemic. | |||||
| AL-SURIMI ET AL. [14] | Assessment of quality of life of HHC patients based on (Physical, Social, Environmental, Psychological) domains. | All (300) HHC patients at National Guard Health Affairs in King Abdul-Aziz Medical City. | Quantitative Retrospective Cross sectional | Using the Arabic version of WHOQOLBREF questionnaire |
Overall total QOL score was 3.78 ± 0.78. |
| Being married and available emotional support affect QOL positively | |||||
| Strokes and psychological problem affect QOL negatively. |
|||||
| ALRUWAILI, LAMEES; ALSAID, TARIQ; AND KOFI, MOSTAFA [15] | Studying risk factors for readmission into hospital among patients of HHC program at PSMMC. | All patients (213) with active file, who are listed in HHC program at PSMMC re-admission within 30 days of discharge. |
Quantitative Retrospective Cross- sectional | Self-administered chart review | Readmission was highest among age group 33-44 at 60% and absent for ages 26-34. |
| Overall readmission was 43.66%, being significantly higher among males at 55.81%. | |||||
| High rates of all-cause readmission exceeded 43% and was significantly associated with male gender, patients with UTI, patients on NGT, functional disability patients, hypothyroidism, a far distance from the central region, and the number of home care days. | |||||
| Poly-pharmacy and diabetes mellitus were the highest frequent causes of readmission | |||||
| ALDAHMASH ET AL. [16] | Demonstration and explanation of the RAHAH connected health system implementation and the challenges facing the process | The components of a RAHAH connected health intervention, and its implementation in Saudi Arabia and Pakistan. | Qualitative Literature Review | Description based on the (TIDieR) checklist. | RAHAH is being implemented as a comprehensive connected health intervention in home healthcare and bariatric surgery departments at KSUMC hospital and gynecology departments at two hospitals. |
| 22 patients have been recruited, out of 40 targeted. | |||||
| Remote devices are used to monitor terminally ill or geriatric patients. | |||||
| The physicians or nurses in the HHC Department, KSUMC, provide instructions demonstrate using the devices. | |||||
| Physicians and nurses from the HHC Department have received appropriate training. | |||||
| ALHARBI ET AL. [17] | Assessment of RSV vaccination status during the COVID-19 pandemic and recommendations for improved vaccination program. | Patients requiring immunization against RSV infection in KSA. | Qualitative recommendations article | Monitoring the status of immuno- prophylaxis against RSV during COVID-19 pandemic | Respiratory syncytial virus mortality is an issue in developing countries, and it can be increased due to COVID-19. |
| Recommendations include increasing RSV immuneprophylaxis program clinics, drive-thru visits, and home vaccinations. | |||||
| Public vaccination status changed due to COVID-19 lockdown and curfew. | |||||
| QURESHI, ET AL. [18] | An attempt to standardize telerehabilitation practice in Saudi Arabia through recommended Guidelines | Rehabilitation professionals | Qualitative recommendations article | Recommended guidelines to facilitate standardization of telerehabilitation care delivery. | Most rehabilitation services are limited to outpatient clinic and are not fully mature. |
| The major problem that there is shortage in bed rehabilitation in hospitals. | |||||
| Apps like TAWAKKALNA were developed to allow medical practitioners to provide HHC. | |||||
| Saudi Arabia does not have standard procedures and protocols for tele-rehabilitation. | |||||
| Tele-rehabilitation guidelines in Saudi Arabia were developed for help rehabilitation practitioners in their work. | |||||
| IBRAHIM KAMIL LUTTFI [6] | Highlighting the importance of adequate training of HHC professionals and providing recommendation to it. | HHC professionals, including physicians, nurses, pharmacists… | Qualitative recommendations article | Discussion on the importance of training and staff development in the Home Health- care department. | Ongoing professional development is an expressed need and expectation for HHC staff across all career stages. |
| Ongoing training, education, and professional development facilitate the transition to practice for HHC staff and also help to ensure competency and quality patient care throughout the span of staff careers. | |||||
| HALAH ALMULLA AND DENA HASSOUNEH [1] | Assessment of nurse’s knowledge and attitude towards HHC and PC, and satisfaction rates among patients. | 24 literature articles on PC and HHC in Saudi Arabia | Qualitative Literature Review | Conducted online search on medical databases | Nurses were found to have low knowledge in PC. |
| Nurses are more likely to assess and report risks of falls in HHC setting. | |||||
| Nurses cultural and linguistic knowledge needs to increase. | |||||
| Family is important in end-life situations. | |||||
| PC is mainly available as inpatient service. | |||||
| Home-based PC is rarely utilized. | |||||
| HHC programs are available but patients prefer hospital-based PC | |||||
| Mean QOL is high in social and environmental domains, and low in physical domain. |
[12] Assessed fatality trends among HHC patients with chronic disease due to infection by COVID-171 19. A high case fatality rate among homecare patients infected with COVID-19 (26.7%) was found, increasing with age. Almost half of their patients were admitted to the hospital for management of COVID173 19, and hospitalized patients had significantly higher case fatality compared to those who were not hospitalized (50% and 5.7%, respectively, p<0.001). A significantly high case fatality rate among homecare patients with diabetes (35.7%, p=0.002), cerebrovascular accidents (50%, p=0.009) and those with epilepsy (80%, p=0.017) was found.
[6] highlighting the importance of adequate training of HHC professionals and providing recommendations to achieve it, emphasized that ongoing professional development is an expressed need and expectation for HHC staff across all career stages. Also, ongoing training, education, and professional development was important to facilitate the transition to practice for HHC staff and also to help ensure competency and quality patient care throughout the span of staff careers.
3.3 Routine Immunization for Children
As a consequence of the measures taken by the Saudi authorities to contain the pandemic, many
children were at risk of missing out on their scheduled routine immunization. This topic was discussed by two articles, namely, [10] and [17].
[10] performed a cross-sectional study on 577 caregivers of children less than 2 years old to assess their fear of having their children infected by COVID-19 if they were to get into a medical facility to get their routine immunization. 90.8% of caregivers were mothers, and about 37% of caregivers had intentionally delayed their children’s vaccination. The study also concluded that most caregivers were inclined to postpone their child’s vaccination out of being infected by COVID-19 or to prevent the exposure of their children to it. Authors emphasize the importance of routine vaccination in children in order to prevent serious illness and because it is the most cost-effective measure against otherwise lethal situations. This is where home vaccination is crucial. When asked about their attitude towards vaccination-at-home service, 82% of caregivers already knew about it, and 17.5% of them used the service during the lockdown. Several reasons for not using the service were given by caregivers, with the most prevalent reason being not knowing about it in 17.9% of them. In Saudi Arabia, authors find, home vaccination is not yet wildly available, but is in an effort to improve the situation are being done by policymakers, pediatricians, and primary care physicians. Promoting these services and offering them to their patients are the main recommendations provided by the authors of this paper to physicians and 200 pediatricians.
[17] handled the topic of vaccination against RSVs. RSV is a serious risk to children affecting 23.5% of children with respiratory disease in Saudi Arabia. The article explains the measures taken by The Saudi Pediatric Pulmonology Association (SPPA) in order to provide Saudi children with vaccination against this class of viruses. Saudi Initiative of Bronchiolitis Diagnosis, Management, and Prevention (SIBRO) was established in July 2018, establishing guidelines that were declared by the SPPA when RSV infection was found to be widespread in the country. However, due to the COVID-19 pandemic, the vaccination status decreased in Saudi Arabia. The authors proposed a list of solutions to provide the vaccine to children in spite of obstacles introduced by the pandemic. Among these recommendations, home care was highlighted. Improvement methods for the quality of home care need to be discussed with caregivers, and home vaccinations need to be furthered as they were successful in returning vaccination rates to a value close to their original value prior to COVID-19.
3.4 Quality of Life
[14] studied the quality of life of HHC patients based on (Physical, Social, Environmental, Psychological) domains. Their study was performed using the Arabic version of the world health organization’s “quality of life-brief” questionnaire or WHOQOL-BREF in short. The study gathered data from all 300 patients at the HHC unit of National Guard Health Affairs in King Abdul-Aziz Medical City. In a 1-5 scoring system, the overall total QOL scored by HHC patients was averaged at 3.78 ± 0.78. HHC patients were generally satisfied with their social and environmental conditions and were dissatisfied with their physical and psychological quality of life. The main factors that were found to affect the QOL of HHC patients in a positive manner were marital status and the availability of emotional support, which improved the patient’s overall QOL. On the contrary, strokes and psychological problems had a negative effect on patients’ QOL.
3.5 Telehealth
In order to reduce social contact and ensure the highest level of safety for patients, the ministry of health (MOH) in Saudi Arabia had developed and offered many telehealth surfaces. Telehealth is defined as “the use of telecommunications technology to deliver professional services at a distance by linking clinician to client or clinician to clinician for assessment, intervention, and/or consultation” [21].
MOH offered various telehealth services during the COVID-19 era, these services included different methods and techniques such as smartphone apps, Telephone service for people who are without internet connection, health intervention, and many others. More than 19 mobile apps have been released to provide web-based health services to smartphone users, who constitute 96% of the population [22].
[3] discussed the role of telehealth in speech-language services during the pandemic to help therapists with the challenges that interfere with their communication with their patients. When asked if the therapy sessions had stopped as a response to COVID-19, more than 80% of caregivers’ responses were affirmative. Caregivers reported many reasons for this interruption including difficulty accessing services due to the COVID-19 pandemic crisis, which was the most common cause. Other reported difficulties were closure of clinics and temporarily suspended sessions. Also, fear of infection of the child or parents with COVID-19, home quarantine, and the financial burden due to the pandemic were mentioned. On the other hand, some caregivers did not experience any changes after the covid pandemic and reported continued delivery of services. When asked about the types of services provided by the speech-language pathologists (SLP) during COVID-19, they reported receiving recorded treatment sessions by continuing to have their sessions at the clinic, receiving telehealth sessions, applying therapeutic programs to their children themselves with a little as-needed support from their therapists, SLP home therapy sessions, and receiving counseling sessions via telephone.
[13] assesses the awareness and utilization of telehealth services specifically 937, a free, confidential telephone service that provides medical and administrative health-care services at any time for people who are without an internet connection before and during the COVID-19 outbreak in the KSA. This article found a significant increase in awareness of telehealth during the pandemic (before=46% vs during=78%) while a slight increase in the utilization of this service (before=42% vs during=48%) was found. This could mean that there is no significant association between the awareness about the service and its utilization. But this finding also suggests an increase in public acceptance of the service and provides evidence of an equitable telemedicine service for the population. In the 937- telehealth services, four main sub-services were provided:
1. Medical consultation,
2. Reporting complaints about public and private health facilities,
3. Appointment requests for primary health centers and smoking cessation clinics, and
4) Responding to inquiries such as requesting information about infectious diseases, toxins, medicines and providing technical support for MOH mobile apps. It also clarified the Factors that help in Increase the Awareness or Utilization of the 937-Telephone Health Service: gender as women is generally more aware of the service as well as the area of residence where despite there was a notable increase in awareness across all areas in the KSA after the COVID-19 pandemic. the Eastern region showed the maximum increase in awareness from 77% before to 89% during the COVID-19 pandemic. 937-telehealth service includes a specific subservice for hearing impairment patients and deaf people through a special mobile app “ISHARA” (“sign”), through which patients can be connected to the 937-telephone health-care services by a video call with the availability of the sign language sign translation service.
[9] study performed a comparison between inpatient, outpatient and consultation services before and after COVID-19. Comparing medical records of patients in their PC unit, their key finding was that the total admission to PC units did not decrease due to COVID-19. The challenges imposed by the pandemic were overcome by providing support through a virtual clinic and telehealth. Around 87% of their patients were fully satisfied (5/5) with the services provided by the virtual clinic and luckily, there were no positive COVID-19 cases in their healthcare workers in the palliative care department due to the high standard precautions applied at KFMC.
One particularly important intervention that is being developed in KSA is the Remotely Accessible Health-care at Home (RAHAH) connected health. [16] in their article about RAHAH demonstrate and explain implementation of this novel service, and the challenges facing the process. The main goal of this service is to promote remote monitoring, treating and education of the patients, those needing long-term care in particular. In detail explanation of the process, equipment and training courses are provided in the article. The RAHAH intervention includes professional training for technical support, physicians, nurses and a whole spectrum of telehealth providers. It will also include a database for patients’ medical records and relevant data. Remote devices are used to monitor terminally ill or geriatric patients through the RAHAH service. A trial of RAHAH was performed at the HHC Department at KSUMC, Riyadh. The trail involved 22 patients into a three-step program for implementing RAHAH intervention. 1. Patient enrollment, 2. Training to the patients/visitors and 3. Remote patient monitoring. The results of this intervention were very promising, as patients and physicians used RAHAH to improve the patient’s health monitoring and management via the internet. Due to COVID-19 lockdown and restrictions, RAHAH became a very useful tool for providing health support for patients without the risk of exposure to the virus.
A final step to completely adapt the telehealth technology is to have the technology itself, its practice and its providers on the same page. This called for a standardized overall guideline, a need which was addressed by [18]. In their article, Qureshi, et al. attempt to standardize the telerehabilitation practice in Saudi Arabia including almost every aspect of the telehealth service in general. Through this effort, the authors note that most rehabilitation services are limited to outpatient clinics and are not fully mature. The legal challenges and aspects of telemedicine in Saudi Arabia were not well investigated, thus; guidelines were developed to help rehabilitation practitioners in their work.
This article covered several aspects of telemedicine practice. A set of administrative guidelines was proposed, especially concerning medical records management. Another set of guidelines for clinical practice was suggested. It consisted of measurements to ensure informed consent, proper patient evaluation and examination, as well as follow-up and care coordination. A section handling the face-to297 face versus telehealth consultation guidelines was also included. As for equipment, infection control and data policy and procedure, a group of technical guidelines was formed. Ethical considerations were also discussed including several situations such as end-of-life decisions and religious and cultural norms. Finally, a section on special considerations was added, focusing on readiness for pandemics and disaster situations, namely COVID-19 pandemic.
3.6 Finance and marketing
3.6.1 Public Sector
We have found six public (government based) hospitals in the Kingdom of Saudi Arabia that provide home healthcare services, of them 4 are located in the capital city of Riyadh, two in Jeddah and one in Tabuk. These hospitals are mostly located in the large and densely populated cities of the kingdom, however; we have found that King Salman Armed Forces Hospital offers HHC services in the somewhat remote and small city of Tabuk. To add, all of these hospitals established their HHC programs well before the outbreak of the COVID-19 pandemic with establishment dates ranging from 1994-2016. We have also found that these hospitals all provide a wide range of services that fall under the scope of HHC. Three hospitals offer palliative care as part of their HHC program. Four hospitals offer nursing-based services. One hospital (King Abdullah Specialized Children’s Hospital) specializes in offering HHC services to children. Five hospitals offer respiratory care. Four hospitals offer at-home intravenous infusion services. Two hospitals offer wound care. All the hospitals offer general medical care services, with one hospital offering referrals and lab services. Two hospitals offer enzyme therapy. Three hospitals offer nutritional and dietary services. These hospitals also offer niche services such as physiotherapy etc… however, none of them share in the providing of these unique services [23, 24].
3.6.2 Guideline to applying to public HHC
We have found that the Ministry of Health (MOH) of the Kingdom of Saudi Arabia provides an online platform for home healthcare applications. This platform offers a database of public hospitals that provide home healthcare and assigns the patient a facility based on the requested service as well as the nearest location to the patient. In order to access such service, the patient must provide a medical report of no less than 3 months, a photocopy of their national ID and a photocopy of the treatment plan. Once the paperwork is submitted, a healthcare provider will be sent to stay with the patient at home to assess their health status and need for HHC. If requirements are fulfilled, the request shall be considered. Once accepted, the patient shall receive a visit within a week, in order to determine his or her needs. This service can also be accessed inside the hospital if the patient is currently admitted. In order to access this service, the patient is referred by the hospital to their Home Healthcare Department, this referral will indicate the patient’s condition, and the type of service required 72 hours before discharge. Afterwards, an initial assessment of the patient’s condition is conducted by the Home Healthcare Department, the patient will then be visited a week after discharge for a final assessment. Once all criteria are met, the patient’s home care needs will be met within a week [23, 24].
3.6.3 Private Sector
Also, private companies that provide very large services and telehealth were found, for example, applications that help citizens get their service at home. A revolution in the HHC private sector was detected, especially in the number of companies. Before COVID-19 outbreak there were a few private companies that provide home healthcare, however, after the pandemic there was a slight increase in the number of private companies that provide home healthcare services. 12 Private HHC firms were identified, most of them (9 companies) were centered in the capital Riyadh, and 3 companies located in the second most populated city, Jeddah. Each company had its own HHC program and services. Most of them offer similar services, but some offer their clients extra services. Prior to the COVID-19 pandemic, all companies provided the traditional HHC service package including primary care, nursing service, physiotherapy and rehabilitation service, mother and child care, infant care, elderly care, adult care, cancer care, respiratory service, nutrition, critical care, diabetic care, hypertension care, bedsore care and sleep test. On the other hand, after the pandemic, increasing demand for HHC services prompted the establishment of several new services. These services included doctor at home, injection at home, laboratory at home, wound care, X-ray image, specialized clinic, consultations, and COVID-19 testing in addition to the already-available package mentioned above.
23% of companies provided “Doctor at home” service, which was the most expensive service, offering a physician’s visit to assess or diagnose patients. This service came in handy with the strict curfew that was applied in Saudi Arabia in order to contain the pandemic. Nursing at home was a more affordable solution adapted by 53% of companies. 46%. Companies provided laboratory at home service, offering skilled nurses that were sent to the patient home to collect laboratory samples. 23% of companies provided injections at home whether they were simple needles or IV fluids and drugs. 23% of companies provided wound care, which offered a general physician sent to the patient to assist in their wound and care for it. 15% of companies provide X-ray service. This service Is not offered by all companies because the X-ray portable device is very expensive, which limits this service to those who can afford it. Unfortunately, specialized clinics are only provided by one company. COVID-19 PCR testing at home is only provided by one company and which was a shock because this service is not expensive and must be provided by all companies. There are many services like elderly, adult and child care which are offered by 53% of companies. 30% of companies provided diabetic care, while; 15% of the companies provided hypertension care. Sleep testing is provided by one company due to its high cost.
4. Discussion
This systematic review assesses the impact of COVID-19 on the home health-care and palliative care sectors in Saudi Arabia. Starting with 400 papers then filtration according to specific inclusion and exclusion criteria we finally include 13 papers in the review. All of the papers are related to home health367 care, palliative care, and telehealth in Saudi Arabia.
The home health-care system was established in 1991 at King Faisal Specialist Hospital [25] and by that time it had been exposed to many changes and showed large developments in a wide range of services in the healthcare sector. However, in the time before the COVID-19 pandemic began, the development of HHC and palliative care sectors in Saudi Arabia was slow and not well utilized by citizens in the kingdom. As the pandemic began to surface, nation-wide curfews and many social distance protocols were set in place and as a result, the home health-care and palliative care sectors have shown very large developments in their services and an improvement in the awareness and utilization by the kingdom’s citizens. Correspondingly, French experience also shows that home health has been unprecedentedly solicited to relieve the pressure on hospitals during the COVID-19 area [26].
Fear of hospitals as environments of COVID-19 infection guided mothers to postpone their children’s vaccination, which will expose these children to serious illness. This was solved by home service vaccination programs supplied by policymakers, pediatricians and primary care physicians. To add, the Saudi Pediatric Pulmonology Association (SPPA) established the Saudi Initiative for Bronchiolitis Diagnosis, Management, and Prevention (SIBRO) in 2018, and Alharbi et al. [17] proposed a list of solutions to provide the vaccine to children in spite of obstacles introduced by the pandemic, which indicates the awareness of the Saudi medical community and healthcare providers about the danger of postponing vaccinations. In the USA and Canada, fear and avoidance of healthcare workers is a widespread, under385 recognized problem during the COVID-19 pandemic. Taylor et al. suggests that it is associated with the COVID Stress Syndrome and might be reduced by interventions targeting this syndrome [27].
Modern day advanced technology and the internet have provided a major role in the process of providing remote health-care, and this was evident during the period of the COVID19 pandemic. The COVID-19 pandemic has resulted in a considerable expansion of telehealth services in Saudi Arabia as the MOH offered over 19 smartphone applications as well as telephone services for people without internet. Not only did the COVID 19 pandemic increase telehealth services, it increased the awareness and utilization of these technologies by Saudi Arabia’s citizens too. Similarly, the COVID-19 pandemic has resulted in a significant boost in telehealth services in the United States, which has facilitated care for a broad range of conditions and improved patient outcomes [28].
A special and novel service established in KSA specifically was Remotely Accessible Health-care at Home (RAHAH), which is a service that promotes remote monitoring, treating, and education of patients along with monitors for terminally ill or geriatric patients. The trial of RAHAH was very promising, as patients and physicians used RAHAH to improve patient health monitoring and management via the internet, which also proved the increase in awareness and utilization of home health-care and palliative care by Saudi citizens. A similar system is implemented in Mexico, as according to Mendoza 2022, remote healthcare programs have shown the potential to support the health system. The implementation of this pandemic management program impacted the number of consultations given remotely, resulting in effective triage [29].
The public health sector is the KSA has shown progressive growth in the past 30 years and their HHC facilities were no stranger to the trend. As time passes, more and more public hospitals implement HHC regimens with a wide range of services. To add, with the COVID-19 outbreak, these pre-existing HHC facilities seemed to expand their service options with most public hospitals providing respiratory care and some providing specialized care to infants and children as a response to the pandemic. All public-sector hospitals that provide HHC services in the KSA share a government-based online platform and in-person application form for those in need of these services. The online platform has proven to be simple and easy to use for the general public as it is easy to navigate to on the internet and to fill in data, in a straightforward step without any complex procedures. To add, public hospitals also offer an in-hospital admission for HHC services if the online form is not sufficient enough, thus making HHC service access easy and simple for the majority of the population. Furthermore, the eligibility criteria set by the MOH make a wide range of citizens eligible for HHC programs across public hospitals in the kingdom as they aim to enroll the eligible patient in the nearest and most equipped hospital according to their HHC needs.
On the other hand, the private health firms in KSA showed very rapid growth in the number of companies that provide home health care after the COVID-19 pandemic. This review concluded that one company provided new services such as COVID-19 PCR testing, this was an unusual finding given the importance of this service during the pandemic and its relatively low cost. Furthermore, more than half of the companies provide child, adult and elderly care which has become an important part of HHC services due to increased awareness regarding home health care in the KSA. To add, almost half of the companies provide laboratories at home which is a very helpful service in saving both money and time. Many companies provide diabetic care at home, and this service is used frequently as diabetes is highly prevailing illness in Saudi Arabia [30].
During the era of the pandemic, few companies developed doctor at home services which is a new field in the home health care sector. Many companies also provide wound care and post-surgical wound care, this service is important and must be used frequently to prevent any wound infection. Very few companies provide hypertension, X-ray and sleep test services in comparison to the population size, which is odd, since these services are essential for a wide range of diseases that could affect the general public.
5. Conclusion
We conclude that COVID-19 has a great impact on all faces of home health-care sector and palliative as well as it causes a steep increase in both services and awareness of telehealth services. In addition, COVID-19 Contributes to the increase in the number of companies that provide home care surfaces and drive the already excitant companies to improve their services and introduce new surfaces to cope with curfew and to try to replace hospitals services as much as possible.
Declarations
Ethics approval: since this is the systematic review there for an institutional board or an ethical committee approval was not required.
Funding: None.
Conflicts of interest: The author declare that they have no conflict of interest.
Availability of data and material: All data are available upon request.
Author’s contribution:
SM: Conceptualization and Senior Review.
MA, MT, AS, RN: Literature search, and manuscript preparation.
All authors have read and agreed to the published version of the manuscript
References
1. Almulla, H. and D. Hassouneh, Home-Based Palliative Care and Home Health Care in Saudi Arabia: An Integrative Literature Review. Home Health Care Management & Practice. 0(0): p.10848223221085684.
2. Landers, S., et al., The Future of Home Health Care: A Strategic Framework for Optimizing Value. Home Health Care Manag Pract, 2016. 28(4): p. 262-278.
3. Al Awaji, N.N., A.A. Almudaiheem, and E.M. Mortada, Assessment of caregivers’ perspectives regarding speech-language services in Saudi Arabia during COVID-19. PLoS One, 2021. 16(6): p.e0253441.
4. MoH. Healthcare Transformation Strategy 2019 [cited 2022 19th July]; Available from: https://www.moh.gov.sa/en/Ministry/vro/Pages/Health-Transformation-Strategy.aspx.
5. WHO. WHO COVID-19 dashboard. World Health Organization. [cited 2022 July 1st]; Available from: https://covid19.who.int/.
6. Luttfi, I., The importance of training and staff development in the Home Health Care department Ministry of Health, Home Health Care Riyadh KSA Ibrahim Kamil Luttfi-*****************.2022.
7. Obied, D.A., et al., Containment of COVID-19: the unprecedented response of Saudi Arabia. J Infect Dev Ctries, 2020. 14(7): p. 699-706.
8. Moher, D., et al., Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev, 2015. 4: p. 1.
9. AlShehery, M.Z., et al., COVID-19 and Palliative Care Services: Comparative Patterns of Inpatient, Outpatient, and Consultation Services in a Tertiary Care Center in Riyadh. Cureus, 2020. 12(12): p. e11996.
10. Baghdadi, L.R., et al., Impact of the COVID-19 Pandemic Lockdown on Routine Childhood Immunization: A Saudi Nationwide Cross-Sectional Study. Front Pediatr, 2021. 9: p. 692877.
11. Alabbasi, K.H., E. Kruger, and M. Tennant, Long Term Implications of Home Healthcare Management on Mortality in Older Adults with Functional Difficulties in the Saudi Community. Geriatrics (Basel), 2021. 6(4).
12. Alshahrani, F.M., M.M.E. Khalaf, and S.R. Rezk, Outcome of COVID-19 among homecare patients and its relation to chronic diseases. Middle East Journal of Family Medicine, 2020. 7(10): p. 111.
13. Al-Rayes, S.A., et al., Public Awareness and Utilization of 937-Telephone Health Services in the Kingdom of Saudi Arabia Before and During the COVID-19 Pandemic: Longitudinal Study. J Med Internet Res, 2021. 23(7): p. e27618.
14. Al-Surimi, K., et al., Quality of life among home healthcare patients in Saudi Arabia: household based survey. Health and Quality of Life Outcomes, 2019. 17(1): p. 21.
15. Lamees Alruwaili, T.A., Mostafa Kofi, Risk factors for hospital readmission among home health care patients at PSMMC, Riyadh, Saudi Arabia, 2019. Int J Adv Community Med 2021, 2021. 4(2): p. 07-13.
6. Aldahmash, A.M., et al., Implementing a connected health intervention for remote patient monitoring in Saudi Arabia and Pakistan: explaining ‘the what’ and ‘the how’. Globalization and Health, 2019. 15(1): p. 20.
17. Alharbi, A.S., et al., Saudi experts’ recommendation for RSV prophylaxis in the era of COVID-19: Consensus from the Saudi Pediatric Pulmonology Association. Saudi Med J, 2021. 42(4): p. 355- 362.
18. Telerehabilitation Guidelines in Saudi Arabia. Telemedicine and e-Health, 2021. 27(10): p. 1087- 1098.
19. Luttfi, I., The Importance of Accreditation in Home Health Care in KSA. 2018.
20. Alsadaan, N., et al., Challenges Facing the Nursing Profession in Saudi Arabia: An Integrative Review. Nurs Rep, 2021. 11(2): p. 395-403.
21. Association, A.S.-L.-H., ASHA speech-language pathology health care survey issue briefs: Vacancies. ASHA speech-language Pathol. Heal. care Surv. issue briefs Vacanc. MD Author, 2005.
22. Hassounah, M., H. Raheel, and M. Alhefzi, Digital Response During the COVID-19 Pandemic in Saudi Arabia. J Med Internet Res, 2020. 22(9): p. e19338.
23. GOV.SA. Home Medical Care. 2021 [cited 2022 10th June]; Available from: https://www.my.gov.sa/wps/portal/snp/servicesDirectory/servicedetails/12424/!ut/p/z0/04_Sj9CPykssy0xPLMnMz0vMAfIjo8zivQIsTAwdDQz9LQwNzQwCnS0tXPwMvYwN3A30g1Pz9L30o_ArAppiVOTr7JuuH1WQWJKhm5mXlq8fYWhkYmSiX5DtHg4Ay6yLtA!!/.
24. MoH. Home Health Care Services 2022 [cited 2022 10th June]; Available from: https://www.moh.gov.sa/en/awarenessplateform/Patientsrights/Pages/HomeHealthCare.aspx.
25. Almoajel, A., et al., THE QUALITY OF HOME HEALTHCARE SERVICE IN RIYADH/SAUDI ARABIA. 2016. 5.
26. Brocard, E., et al., COVID-19’s impact on home health services, caregivers and patients: lessons from the French experience. Lancet Reg Health Eur, 2021. 8: p. 100197.
27. Taylor, S., et al., Fear and avoidance of healthcare workers: An important, under-recognized form of stigmatization during the COVID-19 pandemic. J Anxiety Disord, 2020. 75: p. 102289.
28. Demeke, H.B., et al., Telehealth Practice Among Health Centers During the COVID-19 Pandemic -United States, July 11-17, 2020. MMWR Morb Mortal Wkly Rep, 2020. 69(50): p. 1902-1905.
29. Mendoz, R.L., et al., Remote Healthcare Program in Mexico in the Context of the COVID-19 Pandemic. Healthc Inform Res, 2022. 28(2): p. 152-159.
30. Albarakat, M. and A. Guzu, Prevalence of type 2 diabetes and their complications among home health care patients at Al-Kharj military industries corporation hospital. Journal of Family Medicine and Primary Care, 2019. 8(10): p. 3303-3312.
31. Mukhtar, A., M. Shukry, and D. Bannan, Safe handling and delivery of biological medications during the COVID-19 pandemic. Journal of Clinical Pharmacy and Therapeutics, 2021. 46(4): p.1071-1082.
32. MoH, Statistical Yearbook 2018, ed. K. Ministry of Health. 2018: Ministry of Health, KSA.
33. Walters, M.E., et al., Development of a training programme for home health care workers to promote preventive activities focused on a healthy lifestyle: an intervention mapping approach. BMC Health Services Research, 2015. 15(1): p. 263.
34. Fikar, C. and P. Hirsch, Home health care routing and scheduling: A review. Computers & Operations Research, 2017. 77: p. 86-95.
35. Ahlner-Elmqvist, M., et al., Characteristics and quality of life of patients who choose home care at the end of life. J Pain Symptom Manage, 2008. 36(3): p. 217-27.
© Copyright 2023, All Rights Reserved. Use of this content signifies your agreement to the T&Cs of Unified Citation Journals
This abstract of Manuscript/Paper/Article is an open access Manuscript/Paper/Article distributed under the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/) which allows and permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited and accepted.
This communication and any documents, or files, attached to it, constitute an electronic communication within the scope of the Electronic Communication Privacy Act (https://it.ojp.gov/PrivacyLiberty/authorities/statutes/1285)
To citation of this article: Suha Matar, PGD,CPHRM,RN¹*, Mohammad T. Abuawwad², Mohammad J. J. Taha², Ayham R. K. Sara², 4 Rakan Munif Nassralla², Impact of COVID-19 on Home Health-Care Sector in Saudi Arabia: A Systematic Review, Global Journal of Medical & Clinical Case Reports & Studies